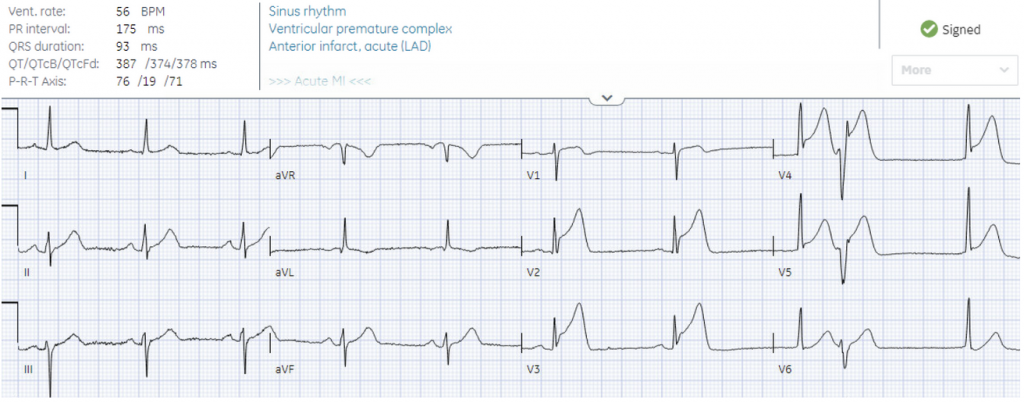
–Heart rate/rhythm: sinus brady with PVC
–Electrical conduction: normal intervals
–Axis: normal
–R-wave progression: early
–Tall/small voltages: normal
–ST/T changes: primary ischemic STE and hyperacute waves V2-5, terminal QRS distortion V3, excess discordant STE in V4 PVC, subtle inferior STD reciprocal to STE in V1. There is no inferior STD and instead possible hyperacute T waves in II/aVF STE